
More Information
Submitted: May 25, 2026 | Approved: June 16, 2026 | Published: June 17, 2026
Citation: Chakraborty T, Siddiqua N, Trisa SS, Anwar SF, Akbar GW. Human Poxvirus Infections: Epidemiology, Transmission, and Clinical Features of Major Orthopoxvirus Diseases. Int J Clin Microbiol Biochem Technol. 2026;9(1): 34-39. Available from:
https://dx.doi.org/10.29328/journal.ijcmbt.1001038
DOI: 10.29328/journal.ijcmbt.1001038
Copyright license: © 2026 Chakraborty T, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Orthopoxvirus; Monkeypox (MPXV); Smallpox; Cowpox; Molluscum contagiosum

Human Poxvirus Infections: Epidemiology, Transmission, and Clinical Features of Major Orthopoxvirus Diseases
Trisha Chakraborty, Naima Siddiqua, Subrin Shabab Trisa, Syeda Fatima Anwar and Gazi Wafa Akbar*
Department of Biochemistry and Biotechnology, University of Science and Technology Chittagong, Chattogram – 4202, Bangladesh
*Corresponding author: Gazi Wafa Akbar, Department of Biochemistry and Biotechnology, University of Science and Technology Chittagong, Chattogram – 4202, Bangladesh, Email: [email protected]
Poxviruses are big, double-stranded DNA viruses that can infect a variety of animal hosts, including humans. Other clinically significant poxvirus infections, such as monkeypox (mpox), cowpox, and molluscum contagiosum, continue to present new and re-emerging public health issues even after smallpox was eradicated. The epidemiology, transmission dynamics, clinical manifestations, diagnostic methods, and treatment approaches of the four main human poxvirus infections are all covered in this study’s methodical narrative synthesis.
Relevant studies published between 2000 and 2025 were found by a systematic search of PubMed, Scopus, and Google Scholar; 34 of them were included in the final analysis. Results show that poxviruses differ significantly in host range, transmission patterns, and disease severity, despite sharing common biological traits including cytoplasmic replication and distinctive cutaneous lesion progression. While mpox has resurfaced worldwide, exhibiting persistent human-to-human transmission during the 2022–2023 outbreak, smallpox is still historically relevant because of its high fatality and successful eradication. Cowpox is still an uncommon zoonotic disease associated with animal reservoirs, while Molluscum contagiosum is still very common, especially in children and immunocompromised people. Antiviral medications like tecovirimat offer treatment options for severe cases, and advances in molecular diagnostics, especially polymerase chain reaction, have improved detection.
The impact of dwindling population immunity and growing human-animal interaction is demonstrated by the resurgence and persistence of poxvirus diseases. To reduce future epidemics, more surveillance, better diagnostic capabilities, and integrated One Health policies are crucial.
Poxviruses are among the largest and most complex double-stranded DNA (dsDNA) viruses that can infect humans and a variety of animal hosts, including insects, birds, and mammals. They are members of the Poxviridae family, which is roughly divided into two subfamilies according to host specificity: Entomopoxvirinae, which infects invertebrates, and Chordopoxvirinae, which infects vertebrates [1,2]. Members of this family are distinguished by their enormous linear dsDNA genomes, which range from 130 to 260 kilobase pairs, and by their characteristic brick-shaped morphology, measuring about 200-300 nm [3]. Poxviruses, in contrast to most DNA viruses, replicate entirely within the cytoplasm of infected host cells and encode several enzymes required for their own transcription and replication [4].
Several genera, especially Orthopoxvirus and Molluscipoxvirus, are of significant medical significance within the Chordopoxvirinae subfamily. The variola virus, which causes smallpox, the monkeypox virus (MPXV); and the cowpox virus are all members of the Orthopoxvirus genus. These viruses have important genetic and antigenic similarities that allow for cross-protective immunity [5]. The molluscum contagiosum virus (MCV), on the other hand, is a frequent, benign cutaneous infection that only affects humans and is part of the Molluscipoxvirus [5]. These viruses display conserved biological traits, such as comparable replication mechanisms and distinctive skin lesion progression, despite variations in host range and pathogenicity.
Poxviruses have historically had a significant impact on human health, especially smallpox, a highly contagious and frequently lethal disease caused by the variola virus. According to research, smallpox first appeared at least 3,000 years [6] ago and persisted as an endemic disease for centuries in various regions of the world, with fatality rates from severe cases as high as 30% [7]. The foundation for modern vaccination was established in 1798 when Edward Jenner showed that cowpox virus inoculation may protect against smallpox [8]. One of the biggest accomplishments in public health was the successful worldwide eradication of smallpox in 1980, resulting from this finding and a vigorous World Health Organization (WHO) vaccine program [6].
Population-level immunity against orthopoxviruses has dramatically decreased since smallpox was eradicated and routine immunization was discontinued. Other zoonotic orthopoxvirus illnesses, such as monkeypox (MPXV), have resurfaced and become more common as a result of this “immunity gap” [9]. MPXV, first detected in humans in the Democratic Republic of the Congo in 1970, has traditionally been seen only in Central and West Africa. However, the extraordinary worldwide outbreak that occurred in 2022-2023 showed persistent human-to-human transmission across several continents [10]. These incidents have brought attention to zoonotic poxviruses’ potential for epidemics in a world growing more interconnected by the day.
Despite being uncommon in humans, the cowpox virus is nevertheless a significant zoonotic pathogen that is mostly spread by contact with infected rodents or domestic animals like cats. Notably, the cowpox virus is thought to be evolutionarily ancient and has one of the biggest genomes among orthopoxviruses. Evidence suggests that other orthopoxviruses, such as variola and vaccinia viruses, evolved by increasing gene loss (reductive evolution) [11]. On the other hand, the molluscum contagiosum virus, which is mainly spread by direct skin-to-skin contact or contaminated surfaces (fomites), is still quite common throughout the world, especially among youngsters, sexually active adults, and immunocompromised people [6].
Poxviruses have been crucial in improving our knowledge of viral pathogenesis, host-virus interactions, and immune responses in addition to their clinical significance. Additionally, antiviral medications like brincidofovir and tecovirimat, which were initially established to prepare for smallpox, are now being used to treat newly emergent illnesses like MPXV [12]. This review offers a comparative synthesis integrating evolutionary dynamics, transmission mechanisms, and clinical features across major human poxviruses, with special attention to the post-smallpox immunity gap and emerging zoonotic risks, in contrast to earlier studies that mainly focus on individual poxvirus infections.
Thus, the goal of this study is to present a thorough comparative investigation of four medically significant poxvirus infections: molluscum contagiosum, cowpox, smallpox, and monkeypox (MPXV), with an emphasis on their virology, evolution, transmission methods, clinical characteristics, and implications for public health. This review provides an integrated comparative overview of major human poxvirus infections by combining evolutionary, epidemiological, clinical, and public health perspectives.
Overview of the poxviridae family
Poxviruses are giant, enveloped double-stranded DNA viruses belonging to the family Poxviridae that infect both vertebrate and invertebrate hosts. The capacity of poxviruses to replicate completely inside the cytoplasm of infected cells, rendered possible by transcriptional and replication machinery encoded by the virus, is one of their distinguishing characteristics [1,2]. These viruses are among the biggest known animal viruses, with an ovoid or brick-shaped morphology and a size of about 200-300 nm [3]. Their genomes, which vary in size from 130 to 260 kilobase pairs, encode a large number of proteins that are involved in immune evasion, host contact, and replication. (Table 1).
| Table 1: Classification and key biological characteristics of major human poxviruses.The table summarizes the taxonomy, host range, genome size, transmission routes, and major clinical characteristics of medically important human poxviruses. | |||||
| Virus | Genus | Primary host range | Approximate genome size | Major transmission route | Key clinical feature |
| Cowpox virus | Orthopoxvirus | Rodents, cats, humans | ~220 kb | Zoonotic contact | Localized pustular lesions |
| Monkeypox virus (MPXV) | Orthopoxvirus | Rodents, primates, humans | ~197 kb | Direct contact, respiratory exposure | Lymphadenopathy with vesiculopustular rash |
| Variola virus (Smallpox) | Orthopoxvirus | Humans only | ~186 kb | Respiratory droplets | Severe centrifugal rash |
| Molluscum contagiosum virus (MCV) | Molluscipoxvirus | Humans only | ~190 kb | Skin-to-skin contact | Umbilicated papules |
Based on host specificity, the Poxviridae family is separated into two subfamilies: Entomopoxvirinae, which infect insects, and Chordopoxvirinae, which infect vertebrates [2]. The genera Orthopoxvirus and Molluscipoxvirus are the most significant to human health within the Chordopoxvirinae. Variola virus (smallpox), monkeypox virus (MPXV), and cowpox virus are all members of the Orthopoxvirus genus. These viruses have substantial antigenic similarities and cross-protective immunity [5]. The molluscum contagiosum virus (MCV), on the other hand, is a human-specific disease that causes benign cutaneous lesions and is included in the Molluscipoxvirus [5].
The cowpox virus is one of the most genetically complicated orthopoxviruses, which are assumed to have evolved from a common ancestor. It is thought that reductive evolution involving gene loss and host adaptation is how other orthopoxviruses, such as variola virus, evolved [11]. The host range, virulence, and transmission patterns of poxviruses vary due to these evolutionary changes.
The primary human poxvirus infections - cowpox, smallpox, monkeypox (MPXV), and molluscum contagiosum - were the participants of this study’s narrative comparative analysis of published literature. The PubMed, Scopus, and Google Scholar databases were searched electronically to identify pertinent literature published between 2000 and 2025.
The keywords “poxvirus”, “orthopoxvirus”, “monkeypox”, “mpox”, “cowpox”, “smallpox”, “molluscum contagiosum”, “epidemiology”, “transmission” “clinical manifestations,” “diagnosis,” “treatment”, and “public health” were all combined in the search strategy. Search phrases were combined and refined using Boolean operators (AND/OR).
Inclusion criteria were peer-reviewed original articles, outbreak investigations, epidemiological studies, clinical studies, review articles, and pertinent systematic reviews addressing the virology, epidemiology, transmission, diagnosis, treatment, or clinical features of human poxvirus infections. Duplicate publications, conference abstracts without full text accessibility, articles published in languages other than English, and animal-only studies with no direct human relevance were all disqualified.
After first screening titles and abstracts for relevance, possibly eligible publications were evaluated in full. The included literature comprised narrative reviews, systematic reviews, observational studies, outbreak investigations, epidemiological surveillance reports, and clinical case series related to major human poxvirus infections. Insufficient relevance to human poxvirus infections, a lack of clinical or epidemiological data, duplicate findings, or inaccessible full text were the reasons why articles were removed during full-text review. To present a comparative overview of the epidemiological patterns, transmission dynamics, clinical manifestations, and public health consequences of major human poxvirus infections, data from the chosen studies were narratively assembled. The study selection process is summarized in Figure 1.
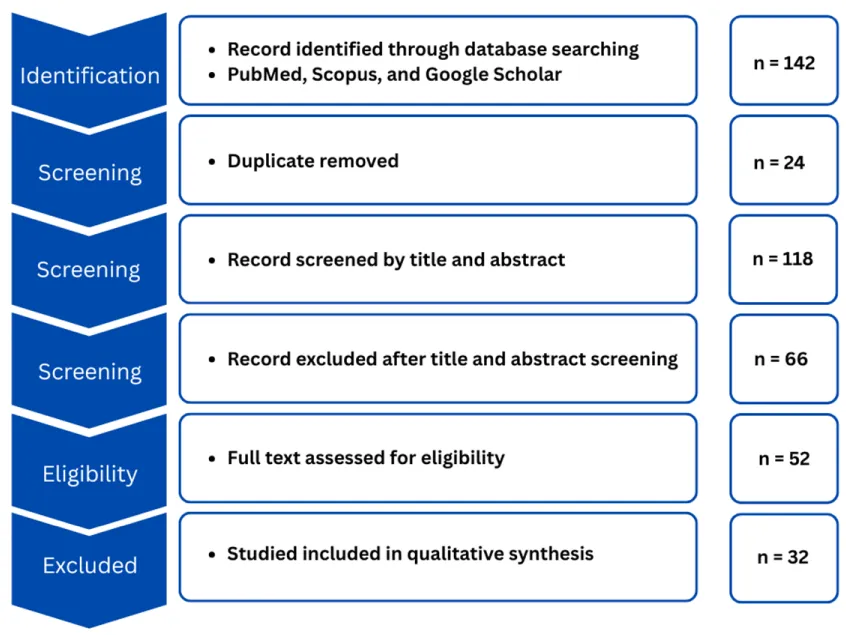
Figure 1: Flow Diagram of Literature Search and Study Selection Process. The diagram summarizes the identification, screening, eligibility assessment, and inclusion of studies included in the qualitative synthesis of major human poxvirus infections.
A total of 142 records were identified through database searching. After removal of duplicates, 118 records remained. Following title and abstract screening, 74 articles were retained for further assessment. Of the 52 full-text articles evaluated for eligibility, 32 articles met the inclusion criteria and were included in the final review (Figure 1).
The included studies comprised review articles, outbreak investigations, epidemiological studies, and clinical studies focusing on major human poxvirus infections. Findings were synthesised to evaluate epidemiological patterns, transmission dynamics, clinical manifestations, diagnostic approaches, and treatment strategies associated with cowpox, smallpox, monkeypox (MPXV), and molluscum contagiosum.
Epidemiology and transmission
These findings indicate that direct contact with lesions and zoonotic exposure are the dominant transmission pathways [6,9,10]. Indirect transmission via fomites, including clothing and bedding, was also frequently documented due to the environmental stability of these viruses [10].
Zoonotic transmission was identified as a major pathway for cowpox and monkeypox infections, with rodents and small mammals acting as primary reservoirs [9-11,13,14]. In contrast, the variola virus and molluscum contagiosum virus were reported to be restricted to human hosts [5,15]. Smallpox historically demonstrated highly efficient respiratory transmission, whereas monkeypox exhibited more limited respiratory spread, requiring prolonged close contact [10,16]. Molluscum contagiosum transmission was predominantly associated with direct skin-to-skin contact and contaminated surfaces [5,15]. A summary of the transmission characteristics of major human poxviruses is presented in Table 2.
| Table 2: Comparative Transmission Characteristics of Major Human Poxviruses. The table highlights reservoir hosts, common epidemiological characteristics that influence disease development, and key transmission routes (zoonotic, human-to-human, fomite, and respiratory). | |||||
| Disease | Primary transmission route | Natural reservoir | Direct contact | Fomite transmission | Respiratory transmission |
| Cowpox | Zoonotic (animal-to-human) | Rodents (primary), cats (intermediate) | Contact with animal lesions | Possible | Rare |
| Molluscum Contagiosum | Human-to-human | Humans | Skin-to-skin contact; sexual transmission | Common (towels, clothing) | Not reported |
| Monkeypox (MPXV) | Zoonotic + human-to-human | Rodents, small mammals | Contact with lesions, body fluids | Yes (bedding, surfaces) | Limited (prolonged exposure) |
| Smallpox (Variola) | Human-to-human | Humans only | Contact with lesions or fluids | Yes | Major route (highly efficient) |
| Abbreviations: MPXV, Monkeypox virus; MCV, Molluscum contagiosum virus. “Limited respiratory transmission” indicates transmission requiring prolonged close exposure. | |||||
Recent studies highlighted shifts in epidemiological patterns following smallpox eradication, including the increasing prominence of zoonotic and re-emerging orthopoxvirus infections [8-10]. The shared epidemiological characteristics underlying poxvirus transmission are summarised in Table 3. The 2022-2023 MPXV outbreak demonstrated sustained human-to-human transmission beyond endemic regions, often associated with close contact and international travel [10,17].
| Table 3: Shared Epidemiological Characteristics Underlying Poxvirus Transmission and Persistence. | |
| Feature | Explanation |
| Lesion-associated viral shedding | High viral load in vesicles, pustules, and scabs facilitates transmission |
| Close-contact requirement | Most infections require prolonged physical contact |
| Environmental stability | Viruses remain viable on surfaces, enabling indirect spread |
| Similar lesion progression | Reflects conserved replication within epithelial tissues |
| Note: Characteristics synthesized from included studies (n = 32). Abbreviations: MPXV, monkeypox virus; MCV, molluscum contagiosum virus. | |
Specific virus profiles
The main human poxvirus infections have different clinical and epidemiological characteristics which are outlined here.
Cowpox: According to studies, the cowpox virus (CPXV) is a zoonotic orthopoxvirus that is mostly maintained in rodent reservoirs. Domestic animals like cats can accidentally infect humans. [11]. Localised pustular lesions, regional lymphadenopathy, and moderate systemic symptoms are common clinical presentations. Immunocompromised people have been documented to experience severe consequences, including ocular involvement [3,11].
Smallpox (Variola virus): A centrifugal pustular rash with synchronous lesion progression and a high fever are the hallmarks of smallpox, a severe human-specific infection [6,7]. Variola major mortality rates ranged from 20 to 45%. Studies repeatedly emphasized the eradication in 1980 after worldwide vaccination campaigns [6,7].
Monkeypox (MPXV): According to reports, MPXV is a zoonotic orthopoxvirus that resides in rodents [9,10,14]. Fever, lymphadenopathy, and a vesiculopustular rash that resembled smallpox but had a lower death rate were among the clinical manifestations [13,14,17-19]. Research from the 2022 pandemic demonstrated persistent transmission from person to person, especially through intimate physical contact [10,17]. Immunocompromised people and children were more likely to report severe illness [16,17].
Molluscum Contagiosum (MCV): MCV was defined as a human-specific virus that causes umbilicated papules and a benign, skin-limited illness [5,15]. Immunocompromised people and children were found to have a high prevalence. Research has shown that lesion persistence is influenced by viral immune evasion mechanisms [5,15].
Clinical manifestations
Poxvirus infections usually cause a distinctive series of skin lesions, starting with macules and moving on to papules, vesicles, pustules, and crusts. However, distinct poxvirus infections differ greatly in terms of location, intensity, and related systemic symptoms.
High fever, lethargy, severe systemic symptoms, and a centrifugal rash with lesions growing simultaneously throughout the body were the hallmarks of smallpox in the past. On the other hand, the symptoms of monkeypox (MPXV), which helps differentiate it from smallpox, include fever, headache, myalgia, and significant lymphadenopathy. The face, limbs, genital area, and mucosal surfaces can all be affected by vesiculopustular skin lesions [14,21,23].
At the site of inoculation, cowpox infections typically present as a single or small number of painful pustular lesions, frequently accompanied by minor systemic symptoms and regional lymphadenopathy. Although severe illness is rare, immunocompromised people may experience it [11].
Small, flesh-colored, dome-shaped papules with central umbilication are the hallmark of Molluscum contagiosum, which is very different from orthopoxvirus infections. Although immunocompromised people may experience widespread illness, lesions are usually asymptomatic and limited to the skin [5,17].
Table 4 presents a comparative overview of the main clinical signs of the most common human poxvirus infections.
| Table 4. Clinical Manifestations and Key Characteristics of Major Human Poxvirus Infections. | |||||
| Virus | Incubation period | Lesion type | Lymphadenopathy | Systemic symptoms | Mortality |
| Smallpox | 7–17 days | Centrifugal pustular rash | Rare | Severe | Up to 30% |
| MPXV | 5–21 days | Vesiculopustular rash | Common | Moderate | Lower |
| Cowpox | Variable | Localized pustules | Common | Mild | Rare |
| Molluscum contagiosum | Weeks–months | Umbilicated papules | Absent | None | None |
This review synthesises current evidence on the epidemiology, transmission, and clinical features of major human poxvirus infections and highlights the increasing importance of zoonotic orthopoxviruses in the post-smallpox era [10,20,21]. Although these viruses share key biological characteristics, including cytoplasmic replication and similar lesion progression, their public health impact varies based on host range, transmission dynamics, and population immunity [3,4,13].
A key finding is the shift in epidemiological patterns following smallpox eradication. The discontinuation of routine vaccination has resulted in a decline in cross-protective immunity against related orthopoxviruses, contributing to an expanding “immunity gap” [8,10,22]. This phenomenon is strongly associated with the resurgence of monkeypox (MPXV), particularly during the 2022-2023 outbreak, which demonstrated sustained human-to-human transmission outside traditionally endemic regions [10,19,23-25].
Zoonotic transmission remains a central driver of emerging poxvirus infections. Cowpox and MPXV are maintained in animal reservoirs, particularly rodents and small mammals, facilitating spillover into human populations [11,21,26-28]. In contrast, the variola virus and molluscum contagiosum virus are restricted to human hosts and primarily spread through close contact and contaminated surfaces [5,15]. The environmental stability of poxviruses further enhances indirect transmission via fomites, contributing to persistence in both community and healthcare settings [3,4].
Clinically, while poxvirus infections share a common pattern of lesion progression, distinct features enable differential diagnosis. Smallpox was historically associated with severe systemic illness and synchronous lesion development, whereas MPXV is distinguished by lymphadenopathy and comparatively lower mortality [13,14,18,29]. Molluscum contagiosum remains a benign, self-limiting condition, while cowpox typically presents as a localised infection [5,15]. These variations highlight the importance of integrating clinical, epidemiological, and laboratory findings for accurate diagnosis.
Molecular diagnostics, especially Polymerase Chain Reaction (PCR), have been useful in detecting poxvirus infections [12,25]. Tecovirimat and Cidofovir have proven to be effective as antiviral drugs mostly against orthopoxviruses such as smallpox and severe monkeypox (MPXV) infections especially in the immunocompromised setting [12,21]. Molluscum contagiosum is however considered to be self-limiting in most of the cases, requiring rarely systemic antiviral therapy [5,17].
From a regional perspective, densely populated and highly connected regions such as South Asia may be particularly vulnerable to emerging outbreaks. Factors including urbanization, population density, and international travel may facilitate rapid transmission if introduced [10,19,22]. Strengthening surveillance systems, enhancing diagnostic capacity, and improving public health awareness are therefore essential.
This review has several limitations. As a qualitative synthesis, it relies on previously published studies, which may introduce reporting bias and heterogeneity in study design. Furthermore, the rapidly evolving epidemiology of MPXV may limit the timeliness of some findings.
Overall, the persistence and re-emergence of poxvirus infections underscore the need for sustained global vigilance. Integrated One Health approaches linking human, animal, and environmental health are critical for early detection and control of zoonotic transmission. Continued investment in surveillance, diagnostics, and targeted interventions will be essential to mitigate future poxvirus outbreaks and their public health impact. The convergence of declining orthopoxvirus immunity, increased human-animal interaction, and global mobility suggests that poxvirus outbreaks may become more frequent rather than sporadic in the coming decades.
Despite the eradication of smallpox, poxviruses continue to pose a significant public health concern, primarily due to the re-emergence of zoonotic orthopoxviruses such as cowpox virus and monkeypox virus (MPXV). The decline in population-level immunity following the discontinuation of routine smallpox vaccination has created an “immunity gap,” increasing susceptibility to emerging and re-emerging orthopoxvirus infections. The recent global spread of MPXV beyond historically endemic regions further highlights the evolving epidemiology and outbreak potential of poxviruses in an increasingly interconnected world.
Addressing these challenges requires strengthened surveillance systems, rapid and accessible diagnostic capabilities, and targeted immunization strategies, particularly for high-risk populations. Enhanced surveillance at the human-animal interface is also critical for the early detection and containment of zoonotic transmission. Moving forward, integrated One Health approaches, combined with continued investment in antiviral development and global preparedness frameworks, will be essential to mitigate future poxvirus outbreaks and reduce their overall public health impact.
Declaration of generative AI and AI-assisted technologies in the manuscript preparation process.
During the preparation of this manuscript, the author used ChatGPT, Grammarly, and QuillBot to improve language clarity, grammar, and overall manuscript rganization. All generated content was critically reviewed and edited by the author, who takes full responsibility for the final content of the manuscript.
- CABI. Poxviridae. CAB International; 2002. Available from: https://www.cabidigitallibrary.org/doi/full/10.5555/20023085623
- Hughes AL, Irausquin S, Friedman R. The evolutionary biology of poxviruses. Infect Genet Evol. 2010;10(1):50-9. Available from: https://doi.org/10.1016/j.meegid.2009.10.001
- Moss B. Poxvirus DNA replication. Cold Spring Harb Perspect Biol. 2013;5(9):a010199. Available from: https://doi.org/10.1101/cshperspect.a010199
- McFadden G. Poxvirus tropism. Nat Rev Microbiol. 2005;3(3):201-13. Available from: https://doi.org/10.1038/nrmicro1099
- Meza-Romero R, Navarrete-Dechent C, Downey C. Molluscum contagiosum: An update and review of new perspectives in etiology, diagnosis, and treatment. Clin Cosmet Investig Dermatol. 2019;12:373-81. Available from: https://doi.org/10.2147/CCID.S187224
- Muyembe-Tamfum JJ, Mulembakani P, Lekie RB, et al. Smallpox and its eradication in the Democratic Republic of Congo: Lessons learned. Vaccine. 2011;29 Suppl 4:D13-8. Available from: https://doi.org/10.1016/j.vaccine.2011.10.049
- Riedel S. Edward Jenner and the history of smallpox and vaccination. Proc (Bayl Univ Med Cent). 2005;18(1):21-5. Available from: https://doi.org/10.1080/08998280.2005.11928028
- Nguyen PY, Ajisegiri WS, Costantino V, Chughtai AA, MacIntyre CR. Reemergence of human monkeypox and declining population immunity. Emerg Infect Dis. 2021;27(4):1007-15. Available from: https://doi.org/10.3201/eid2704.203569
- Ranjan S, Vashishth K, Sak K, Tuli HS. The emergence of mpox: Epidemiology and current therapeutic options. Curr Pharmacol Rep. 2023;9(3):144-53. Available from: https://doi.org/10.1007/s40495-023-00318-y
- Bunge EM, Hoet B, Chen L, Lienert F, Weidenthaler H, Baer LR, et al. The changing epidemiology of human monkeypox. PLoS Negl Trop Dis. 2022;16:e0010141. Available from: https://doi.org/10.1371/journal.pntd.0010141
- Babkin IV, Babkina IN. A retrospective study of the orthopoxvirus molecular evolution. Infect Genet Evol. 2012;12(8):1597-604. Available from: https://doi.org/10.1016/j.meegid.2012.07.011
- Russo AT, Grosenbach DW, Chinsangaram J, Honeychurch KM, Long PG, Lovejoy C, et al. An overview of tecovirimat for smallpox treatment and expanded anti-orthopoxvirus applications. Expert Rev Anti Infect Ther. 2021;19(3):331-44. Available from: https://doi.org/10.1080/14787210.2020.1819791
- Esposito JJ, Fenner F. Poxviruses. J Gen Virol. 2001;82(6):1231-45. Available from: https://doi.org/10.1099/vir.0.19565-0
- Liu Q, Fu L, Wang B, et al. Clinical characteristics of human mpox (monkeypox) in 2022: A systematic review and meta-analysis. Pathogens. 2023;12(1):146. Available from: https://doi.org/10.3390/pathogens12010146
- Likos AM, Sammons SA, Olson VA, Sun Y, Wu X, Peng X, et al. A tale of two clades: Monkeypox viruses. J Gen Virol. 2005;86(10):2661-72. Available from: https://doi.org/10.1099/vir.0.81215-0
- Rimoin AW, Mulembakani PM, Johnston SC, Smith JOL, Kisalu NK, Kinkela TL, et al. Major increase in human monkeypox incidence 30 years after smallpox vaccination campaigns cease in the Democratic Republic of Congo. Proc Natl Acad Sci U S A. 2010;107(37):16262-7. Available from: https://doi.org/10.1073/pnas.1005769107
- Chen X, Anstey AV, Bugert JJ. Molluscum contagiosum virus infection. Clin Dermatol. 2006;24(2):131-9. Available from: https://doi.org/10.1016/j.clindermatol.2005.11.007
- Learned LA, Reynolds MG, Wassa DW, Li Y, Olson YA, Karem K, et al. Extended interhuman transmission of monkeypox in a hospital community in the Republic of the Congo, 2003. Am J Trop Med Hyg. 2005;73(2):428-34. Available from: https://doi.org/10.4269/ajtmh.2005.73.428
- McCollum AM, Damon IK. Human monkeypox. Clin Infect Dis. 2014;58(2):260-7. Available from: https://doi.org/10.1093/cid/cit703
- Damon IK. Status of human monkeypox: Clinical disease, epidemiology and research. Vaccine. 2011;29 Suppl 4:D54-9. Available from: https://doi.org/10.1016/j.vaccine.2011.04.014
- Adler H, Gould S, Hine P, Snell LB, Wong W, Houlihan CF, et al. Clinical features and management of human monkeypox: A retrospective observational study in the UK. Lancet Infect Dis. 2022;22(8):1153-62. Available from: https://doi.org/10.1016/S1473-3099(22)00228-6
- Sklenovská N, Van Ranst M. Emergence of monkeypox as the most important orthopoxvirus infection in humans. Front Public Health. 2018;6:241. Available from: https://doi.org/10.3389/fpubh.2018.00241
- Thornhill JP, Barkati S, Walmsley S, Rockstroh J, Antinori A, Harrison JB, et al. Monkeypox virus infection in humans across 16 countries, April–June 2022. N Engl J Med. 2022;387(8):679-91. Available from: https://doi.org/10.1056/NEJMoa2207323
- World Health Organization. Multi-country monkeypox outbreak in non-endemic countries. Geneva: WHO; 2022. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON388
- Grant R, Nguyen LL, Breban R. Modelling human-to-human transmission of monkeypox. Bull World Health Organ. 2020;98(9):638-40. Available from: https://doi.org/10.2471/BLT.19.242347
- Kumar N, Acharya A, Gendelman HE, Byrareddy SN. The 2022 outbreak and the pathobiology of the monkeypox virus. J Autoimmun. 2022;131:102855. Available from: https://doi.org/10.1016/j.jaut.2022.102855
- Ogoina D, Iroezindu M, James HI, Oladokun R, Yinka-Ogunleye A, Wakama P, et al. Clinical course and outcome of human monkeypox in Nigeria. Clin Infect Dis. 2020;71(8):e210-4. Available from: https://doi.org/10.1093/cid/ciaa143
- Vaughan A, Aarons E, Astbury J, Brooks T, Chand M, Flegg P, et al. Human-to-human transmission of monkeypox virus, United Kingdom, October 2018. Emerg Infect Dis. 2020;26(4):782-5. Available from: https://doi.org/10.3201/eid2604.191164
- Reed KD, Melski JW, Graham MB, Regnery RL, Sotir MJ, Wegner MV, et al. The detection of monkeypox in humans in the Western Hemisphere. N Engl J Med. 2004;350(4):342-50. Available from: https://doi.org/10.1056/NEJMoa032299
- Petersen E, Kantele A, Koopmans M, Asogun D, Yinka-Ogunleye A, Ihekweazu C, et al. Human monkeypox: Epidemiologic and clinical characteristics, diagnosis, and prevention. Infect Dis Clin North Am. 2019;33(4):1027-43. Available from: https://doi.org/10.1016/j.idc.2019.03.001
- Jezek Z, Grab B, Szczeniowski MV, Paluku KM, Mutombo M. Human monkeypox: Secondary attack rates. Bull World Health Organ. 1988;66(4):465-70.
- Kaler J, Hussain A, Flores G, Kheiri S, Desrosiers D. Monkeypox: A comprehensive review of trans-mission, pathogenesis, and manifestation. Cureus, 2022;14(7), e26531. Available from: https://doi.org/10.7759/cureus.26531