
More Information
Submitted: 28 July 2020 | Approved: 10 August 2020 | Published: 11 August 2020
How to cite this article: Mandal M, Mandal S. Estimating global case fatality rate of coronavirus disease 2019 (COVID-19) pandemic. Int J Clin Microbiol Biochem Technol. 2020; 3: 036-039.
DOI: 10.29328/journal.ijcmbt.1001014
Copyright License: © 2020 Mandal M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: COVID-19 pandemic; SARS-CoV-2; Case fatality rate; Global including china; Global excluding china

Estimating global case fatality rate of coronavirus disease 2019 (COVID-19) pandemic
Manisha Mandal1 and Shyamapada Mandal2*
1Department of Physiology, MGM Medical College, Kishanganj-855107, India
2Laboratory of Microbiology and Experimental Medicine, Department of Zoology, University of Gour Banga, Malda-732103, India
*Address for Correspondence: Shyamapada Mandal, Professor, Laboratory of Microbiology and Experimental Medicine, Department of Zoology, University of Gour Banga, Malda-732103, India, Email: [email protected]; [email protected]
Background: There is a huge global loss of lives due to COVID-19 pandemic, the primary epicentre of which is China, where the causative agent of the disease, SARS-CoV-2 was first emerged in December 2019. This study aims to explore the severity, in terms of case fatality rate (CFR), of COVID-19 pandemic.
Methods: Data of ongoing COVID-19 global pandemic were retrieved from website of the WHO, and processed for the estimation of global (both including and excluding China) CFRs of COVID-19. CFRs were explored following the naive estimates, 14-day delay estimates, and linear regression model analysis, during January 25, 2020 to April 25, 2020, on weekly basis. To explore the current situation, in terms of CFR, data for the next 13 weeks (May 2, 2020 through July 25, 2020), were processed by naive and linear regression model analysis.
Results: Mean CFRs, in naive estimates, were 4.59% for the world including China, and 3.62% for the world excluding China. The 14-day delay estimates of CFRs were 15.6% globally, and 21.65% in countries outside China. Following statistical model, global (both including and excluding China) CFRs were 6.81%, by naive estimates, and ~13%, by 14-day delay estimates. Global CFRs of COVID-19 during May 2, 2020 to July 25, 2020, ranged 4.1% – 7.04%, by naive estimates, and by statistical regression analysis the CFR was 3.19%.
Conclusion and recommendations: The CFR might help estimate the need of up-to-date hospital supplies and other mitigation measures for COVID-19 ongoing pandemic, and therefore, instantaneous CFR estimations are recommended.
The world is now witnessing the emergence and global spread of the 21st century’s 3rd deadly coronavirus pneumonia in humans, called COVID-19 (coronavirus disease 2019), caused with the infection of a novel coronavirus, SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) [1]. Notably, the COVID-19 was first seen in December 2019, in Wuhan of Hubei province, China, among a cluster of people linked to the Huanan seafood market, and was emerged zoonotically with a single spillover from animals [2], probably from bat reservoir as had been seen for two other coronaviruses: SARS-CoV (severe acute respiratory syndrome coronavirus) emerged in the Guangdong province, China in 2002, and MERS-CoV (Middle East respiratory syndrome) that emerged in the Arabian Peninsula in 2012, causing SARS and MERS, respectively [3,4].
The COVID-19, which has been declared by the WHO, on March 11, 2020, pandemic, claimed lives at a rate that very rapidly surpassed the cumulative deaths occurred due to SARS and MERS, globally [3-5]. The virus, in addition to the spread from asymptomatic individuals, is within the capacity of showing sustained person-to-person transmission among people in more than 200 countries, wherein persons of all age groups (from children to old people), comorbid patients and people experiencing homelessness are being the target of the novel coronavirus, SARS-CoV-2, which causes COVID-19 in humans [4,6]. As of July 27, 2020, a total of 16,249,165 global COVID-19 cases, including 649,208 deaths, have been reported, since December 31, 2019 [7].
Accounting the above situation, estimating case fatality rate (CFR) would be an important criterion in exploring the severity of the ongoing COVID-19 global pandemic for its containment and mitigation.
The global COVID-19 data were retrieved electronically, on weekly basis for 14 weeks (January 25, 2020 through April 25, 2020), from publicly available domain of the WHO [1]. Since the virus SARS-CoV-2 transmission was contained in China, and the COVID-19 pandemic is evolving in countries outside China, the database was grouped into two clusters: (a) global including China, and (b) global excluding China (i.e., countries outside China). Therefore, the data were processed accordingly in order to calculate CFRs by naive estimates, wherein the number of deaths of COVID-19 patients was divided with the total number of COVID-19 test positive cases, and expressed as percentages [8].
Following the criteria published earlier by others [9,10], the adjusted CFR with 14-day time delay, for 12 consecutive weeks (February 8, 2020 through April 25, 2020) were calculated with the usage of cumulative COVID-19 cases on April 11, 2020, as the denominator, which was 14 days before April 25, 2020 (final week of the study to estimate adjusted CFR), i.e., the date that matched with COVID-19 cases available on April 11, 2020 (and so on).
The data-driven linear regression statistical model analysis was set to estimate CFR, using cumulative COVID-19 cases as the predictor variable, and cumulative COVID-19 deaths as the outcome variable, wherein the goodness of fitting was justified with R2: 0.95-0.99 values [11,12]. The CFRs were calculated following the criteria of naive estimates as well as 14-day delay estimates, for the regions as mentioned above, within this model.
To explore the current as well as advanced status of the global COVID-19 pandemic, in terms of CFR, data for the last 13 weeks (May 2, 2020 through July 25, 2020), retrieved from the WHO website1, were processed by naive as well as linear regression model analysis, as stated above [8,11,12].
Representing the naive estimates curve (CFR: 2.1% – 6.9% for global including China, and 0.35% – 6.94% for global excluding China, during February 8, 2020 through April 25, 2020), the CFRs by 14-day delay estimates were in between 54.8% (on February 8, 2020) and 11.65% (on April 25, 2020) for global including China (range: 5.78-54.8), and 8% (on February 8, 2020) and 58% (on April 25, 2020), for countries outside China; range: 6.64% - 58% (Figure 1).
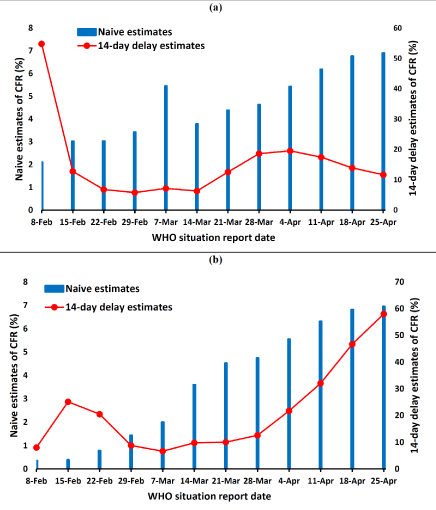
Figure 1: Naive estimates of CFR compared to the adjusted 14-day delay estimates of CFR of COVID-19 (February 8, 2020 through April 25, 2020): (a) global including China; (b) countries outside China.
The mean CFRs, in the naive estimates, were recorded as 4.59% (95% CI: 3.59 – 5.59) in the world including China, and 3.62% (95% CI: 2.01 – 5.23) in the world excluding China. The 14-day delay estimates of CFRs (adjusted CFRs) were 15.6% (95% CI: 7.18 – 24.02) globally, and 21.65% (95% CI: 11.15 – 32.15) in countries outside China. High significance differences between CFRs of the naive estimates and 14-day delay estimates have been noted globally, both including and excluding China (p < 0.001).
The CFRs as estimated following the linear regression statistical model of different regions, according to the criteria for naive estimates as well as 14-day delay estimates, are depicted in figure 2. The global (including China) CFRs were 6.81% (R2: 0.993) following naive estimates criteria, and 12.53% (R2: 0.965), by 14-day delay estimates criteria, while the CFRs as calculated were 6.81% (R2: 0.994), by naive estimates criteria, and 12.67% (R2: 0.956), by 14-day delay estimates criteria, for the world excluding China.
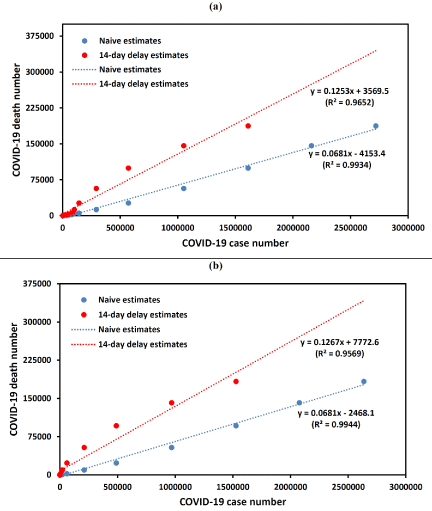
Figure 2: Statistical model analysis of CFR with naive estimates criteria and adjusted 14-day delay estimates criteria for COVID-19 (January 25, 2020 through April 25, 2020): (a) global including China; (b) countries outside China.
The global CFR of COVID-19 as determined for the time period from May 2, 2020 to July 25, 2020, ranged 4.1% – 7.04% (mean: 5.63%; 95% CI: 5.01 – 6.25), by naive estimates (Figure 3a),
while statistical regression model displayed the value as 3.19% with R2: 0.977 (Figure 3b).
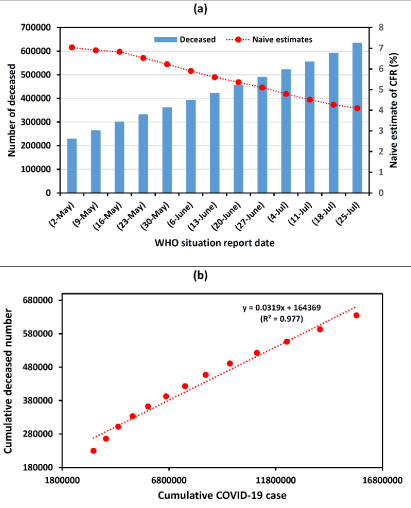
Figure 3: The CFR of global COVID-19 pandemic (May 2, 2020 through July 25, 2020) by (a) naive estimates, and (b) statistical model analysis.
In this communication, as on April 25, 2020, the global adjusted CFR of 11.65% was higher than the CFR of SARS‐CoV (9.6%) [4], while the adjusted CFR of 58% for countries outside China was exceedingly high compared to the CFR of MERS‐CoV (34.4%) [4]. Thus, the adjusted CFRs, as per our estimate, were higher than that of China, as on March 5, 2020 (3.48%), and this is because of the containment of the disease in China, and increasing in the number of cases as well as the mortalities with COVID-19 in countries outside China [1,13].
As of March 3, 2020, the global estimate of COVID-19 CFR has been high (3.4%) compared to the initial estimate of 2% by the WHO, and this was in consonance with 2.3% in China [4]. This is, however, uncertain, since to calculating CFR, dividing the deaths by the cases on a given day of ongoing disease incidences might not the true representative of real CFR estimate (since the undetected asymptomatic cases that also impact on CFR estimation, but were not included). Therefore, to defining the severity of ongoing COVID-19 global pandemic, the estimation of CFR (adjusted CFR), accounting the time delay of 14 days from onset of illness to death, might be an important tool, as explained elsewhere [9,10,13]. However, this model (14-day delay) overestimates the CFR [14,15], as was also seen throughout the current study period.
The 14-delay estimates of CFRs have, therefore, been related to the fact of overestimation of COVID-19 severity [14], and therefore, the data-driven statistical model analysis has been followed to estimate the CFR concerning the ongoing COVID-19 pandemic. Originally, this method was employed for comprehensive CFR estimation of COVID-19, by Yang, et al. [11], and later by Oztoprak, et al. [12], in order to reflect the good estimates of CFRs for different countries. Herein, the estimated CFR for the world (excluding China) and for the countries outside China is similar: 6.81% (by WHO estimates) and ~13% (by 14-day delay estimates), suggesting that the global (excluding China) situation is reasonably scary, considering the fact that China, so far, has effectively controlled the disease (COVID-19), which was caused by the novel coronavirus, SARS-CoV-2, for which there are no specific medicine as well as vaccine [16,17], and therefore, the non-pharmaceutical measures remain the only options for COVID-19 management [18-20]. As per the current report the average CFR of COVID-19 in China was 6.1% that alleviated to 5.7% in April, while the value was recorded as 1% in China excluding Hubei province [21]. Sudharsanan, et al. [22] reported a wide variation in CFRs in the global COVID-19 pandemic recording the lowest values in South Korea (1.6%) and Germany (0.7%) and the highest CFRs in Italy (9.3%) and the Netherlands (7.4%). While China has contained the COVID-19 pandemic it is escalating in rest of the world, however, the disease severity has been improved with a reduction of CFR from 7.04% (on May 2, 2020) to 4.1% (on July 25, 2020), and the value was decreased to 3.19% during May 2, 2020 to July 25, 2020, compared to the value of 6.81% estimated during February 8, 2020 to April 25, 2020, following regression model analysis.
The current findings, combined with the facts mentioned above, reflect the severity, in terms of CFR, of the ongoing COVID-19 global pandemic. Determining weekly as well as the overall CFR values (following naive and statistical model analysis) might help estimate the need for current hospital supplies and other mitigation measures for the ongoing pandemic of COVID-19, for which, no established treatment or a vaccine is available.
Authors’ contributions
MM: Retrieved data, co-wrote and discussed the paper; SM: designed the study, retrieved data, wrote, analyzed data, and discussed the paper.
- World Health Organization. Coronavirus disease (COVID-2019) situation reports. WHO 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/
- Zhou P, Yang X, Wang X, Hu B, Zhang L, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020; 579: 270-273. PubMed: https://pubmed.ncbi.nlm.nih.gov/32015507/
- Peeri NC, Shrestha N, Rahman MS, Zaki R, Tan Z, et al. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: what lessons have we learned? Int J Epidemiol. 2020; 49: 717-726. PubMed: https://pubmed.ncbi.nlm.nih.gov/32086938/
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (covid-19) outbreak in China: summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020; 323: 1239-1242. PubMed: https://pubmed.ncbi.nlm.nih.gov/32091533/
- World Health Organization. WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March. WHO 2020. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19/
- Tsai J, Wilson M. COVID-19: a potential public health problem for homeless populations. Lancet Public Health 2020; 5: E186-E187. PubMed: https://pubmed.ncbi.nlm.nih.gov/32171054/
- European Centre for Disease Prevention and Control. COVID-19 situation update worldwide, as of 27 July 2020. ECDC 2020. https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases/
- Giangreco G. Case fatality rate analysis of Italian COVID-19 outbreak. J Med Virol 2020; 92: 919-923. PubMed: https://pubmed.ncbi.nlm.nih.gov/32297983/
- Baud D, Qi X, Nielsen-Saines K, Musso D, Pomar L, et al. Real estimates of mortality following COVID-19 infection. Lancet Infect Dis. 20; 2020: 773. PubMed: https://pubmed.ncbi.nlm.nih.gov/32171390/
- Linton NM, Kobayashi T, Yang Y, Hayashi K, Akhmetzhanov AR, et al. Incubation period and other epidemiological characteristics of 2019 novel coronavirus infections with right truncation: A statistical analysis of publicly available case data. J Clin Med. 2020; 9: 538. PubMed: https://pubmed.ncbi.nlm.nih.gov/32079150/
- Yang S, Cao P, Du P, Wu Z, Zhuang Z, et al. Early estimation of the case fatality rate of COVID-19 in mainland China: a data-driven analysis. Ann Transl Med 2020; 8: 128. PubMed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7049028/
- Oztoprak F, Javed A. Case fatality rate estimation of COVID-19 for European countries: Turkey’s current scenario amidst a global pandemic; comparison of outbreaks with European countries. EJMO 2020; 4: 149–159.
- Wilson N, Kvalsvig A, Barnard LT, Baker GM. Case-fatality estimates for COVID-19 calculated by using a lag time for fatality. Emerg Infect Dis 26; 2020:1339-1441. PubMed: https://pubmed.ncbi.nlm.nih.gov/32168463/
- Lipsitch M. Estimating case fatality rates of COVID-19. Lancet Infect Dis 20; 2020: 774–775.
- Spychalski P, Błazynska-Spychalska A, Kobiela J. Estimating case fatality rates of COVID-19. Lancet Infect Dis 20; 2020: 775. PubMed: https://pubmed.ncbi.nlm.nih.gov/32243815/
- Jiang S. Don’t rush to deploy COVID-19 vaccines and drugs. Nature 579; 2020: 321. PubMed: https://pubmed.ncbi.nlm.nih.gov/32179860/
- Harrison C. Coronavirus puts drug repurposing on the fast track. Nature Biotechnol 2020; 38: 379-381. PubMed: https://pubmed.ncbi.nlm.nih.gov/32205870/
- Mandal S, Bhatnagar T, Arinaminpathy N, Agarwal A, Chowdhury A, et al. Prudent public health intervention strategies to control the coronavirus disease 2019 transmission in India: A mathematical model-based approach. Indian J Med Res 2020; 151: 190-199. PubMed: https://pubmed.ncbi.nlm.nih.gov/32362645/
- Mandal M, Mandal S. Phasic containment of COVID-19 in substantially affected states of India. medRxiv 2020.
- Mandal M, Mandal S. COVID-19 pandemic scenario in India compared to China and rest of the world: a data driven and model analysis. medRxiv 2020.
- Mia Y, Huanga T, Zhanga J, Qina Q, Gonga Y, et al. Estimating the instant case fatality rate of COVID-19 in China. Int J Infect Dis. 97; 2020: 1–6. PubMed: https://pubmed.ncbi.nlm.nih.gov/32339723/
- Sudharsanan N, Didzun O, Barnighaausen T, Geldsetzer P. The contribution of the age distribution of cases to COVID-19 case fatality across countries. Ann Intern Med. 2020; M20-2973. PubMed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7397549/